
Contraception Is Not the Answer
Free birth control won't move the needle, and better birth control isn't coming.
When commentators are asked what we are to do about the more than two million unintended pregnancies and the slightly less than a million induced abortions that occur every year in the United States, many are apt to give an inoffensive, banal reply describing how we can address this with contraception.
Let us give these comments the benefit of the doubt. There are at least two ways to interpret the comment that contraception can be used to address the issue of unintended pregnancies:
The Lazy Way. The commentator wants to make the contraceptive methods we have now more available.
The Hard Way. The commentator wants to develop new, better contraceptive methods to replace the ones we have now.
The Lazy Way appears in policy debates in the United States over insurance coverage for contraceptives and whether the government should require such coverage.
The reasoning of the Lazy Way makes sense. There is a nontrivial number of couples that conceive an unintended pregnancy every year without using birth control. If such couples used a contraceptive method, they would conceive at a lower rate, and there would be fewer unintended pregnancies. The Lazy Way thinking concludes that we should try to provide these couples access to birth control methods, perhaps at no cost to them.
However, the Lazy Way will almost certainly do nothing. Why? In the United States, people already have abundant access to birth control methods.
Asking the Women It Happened To
The most direct way to get at this is to ask people who conceive an unintended pregnancy when not using any contraceptive method why they did not use a method.
The National Survey of Family Growth (NSFG) asks follow-up questions to female respondents for every pregnancy that is reported as
unintended (i.e., the respondent did not want more/any children or the pregnancy happened too soon),
recent (i.e., the pregnancy ended within the 3 years preceding the interview), and
no contraceptive method was used during the month in which the pregnancy was conceived.1
The text of the question is rendered slightly differently depending on the respondent’s answers to previous questions, but becomes something like the following (emphasis added).
Earlier you told me this pregnancy occurred (too soon / at a time when you wanted no future pregnancies). Which of the following statements applies to you right before you became pregnant this time (that is, with the pregnancy that ended in [DATE]))?
You did not use birth control because...
These questions are asked of a subsample that represented 3,810,000 (±460,000) pregnancies in the 2011–2015 data.2
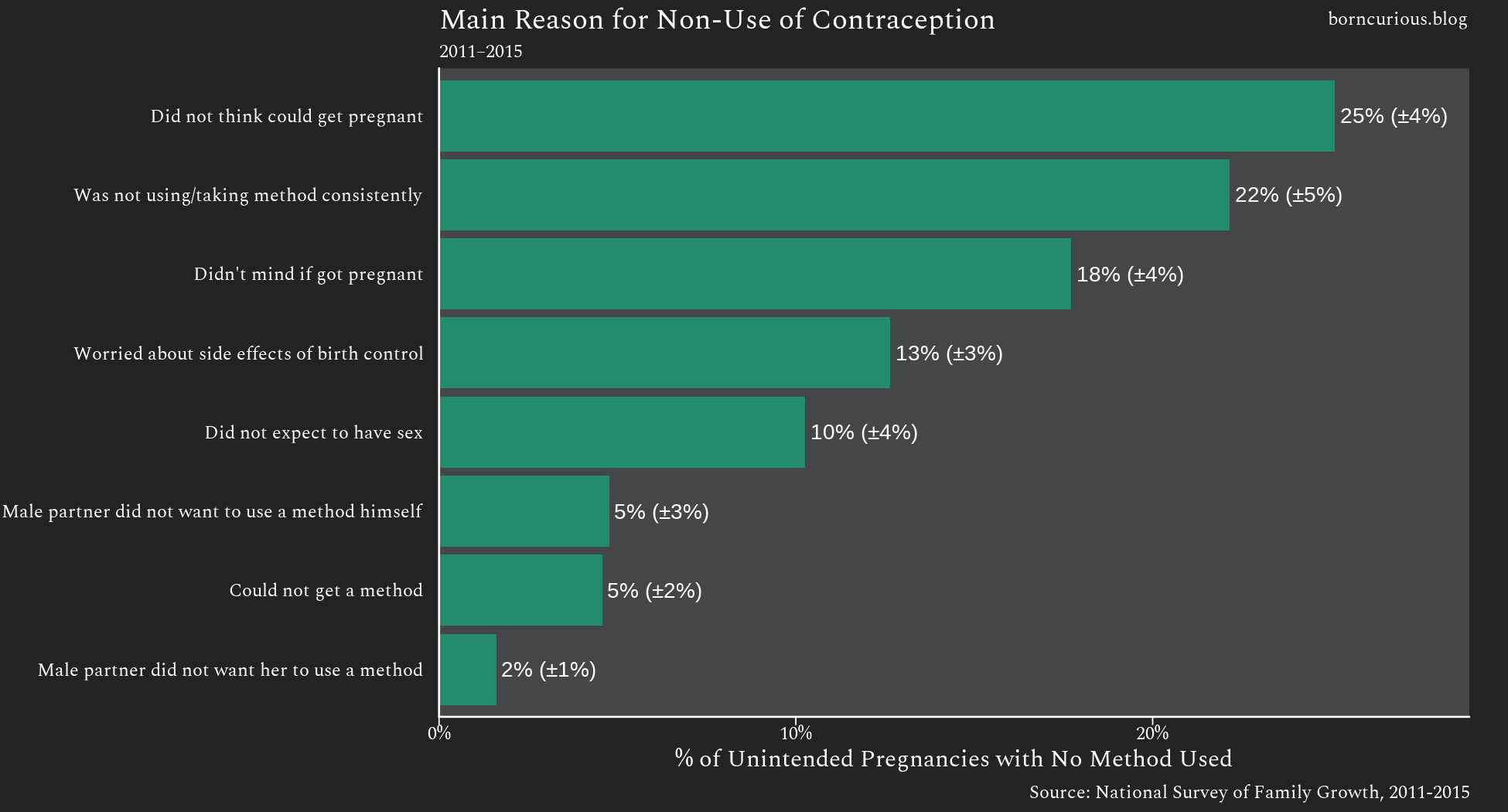
In only about 5% of these pregnancies, the woman reports she could not get a contraceptive method. This accounts for an estimated 174,000 (±77,000) pregnancies out of the 3,810,000.
Indeed, more unintended pregnancies occurred without contraceptive use because of worry about side effects — 482,000 (±140,000) — than lack of access.3 This tracks with how often women discontinue contraceptive methods due to side effects.
Why did I start with 2011-2015 data? Starting in 2015, the NSFG began redacting the specific months when pregnancies began and ended in its public-use files. The NSFG uses an old, long, and complicated instrument. It is thus prone to instrument issues, and I wanted to verify the data, a task that requires the per-month timing of pregnancies.
That being said, similar results come from the 2015-2019 data, which I could not completely check for data integrity issues.
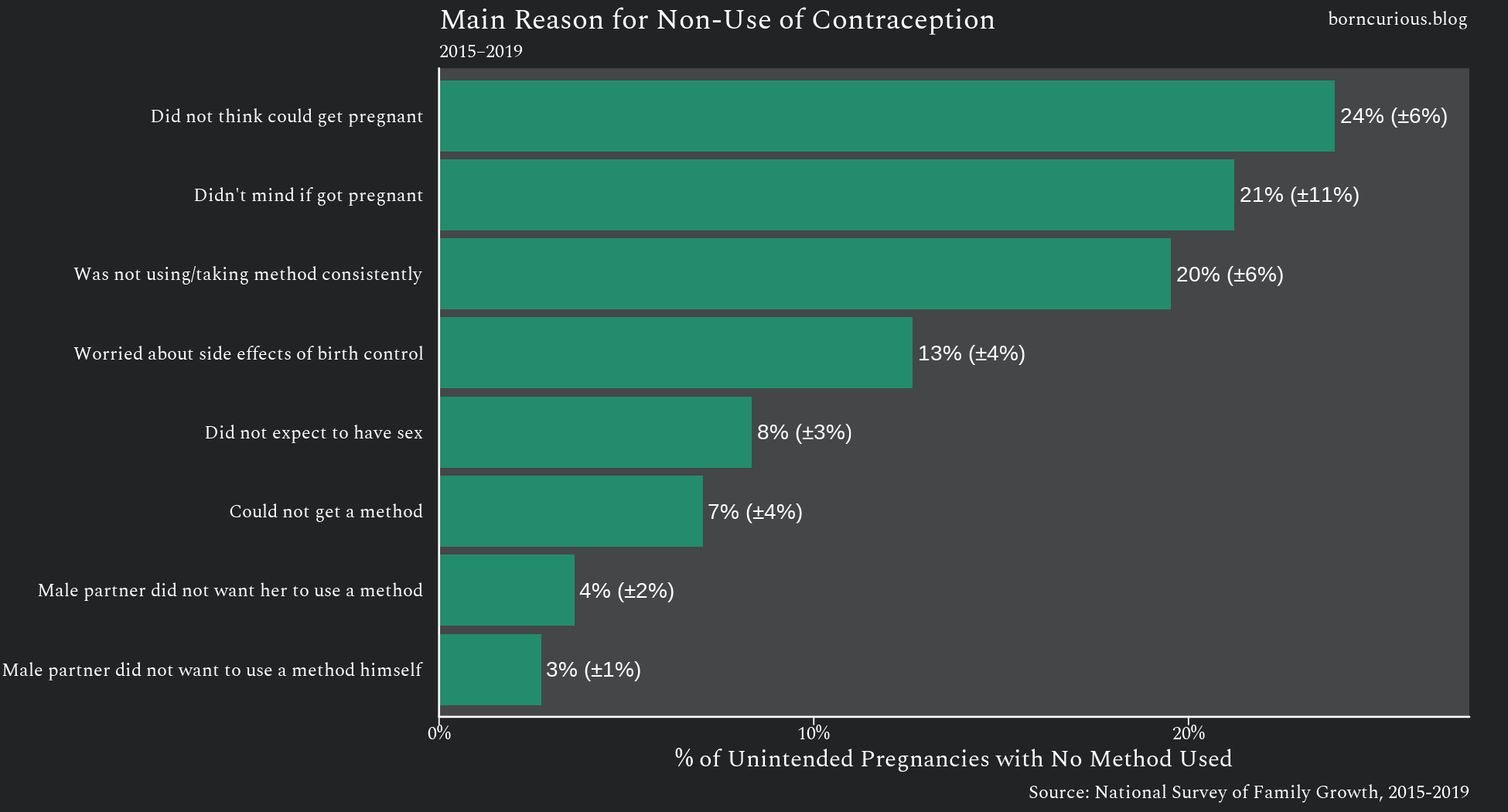
This time around, the subsample represents 3,680,000 (±620,000) pregnancies. The point estimate for “Could not get a method” is slightly greater at 259,000 (±130,000), but with a larger margin of error.4 Differences from the 2011-2015 period are small enough that they could be just sampling error.
Again, the lack of access to contraception is not a substantial issue.
Thus, among those who conceive an unintended pregnancy without using a birth control method, a very small percentage (less than 10%) could not get a method.
Note that “could not get a method” is a bit vague. An even smaller subset of these would have been unable to get a method for financial reasons.
Would They Use Birth Control If It Were Free?
Another approach would be to ask people who are currently not using a birth control method if they would use one, if money were no object. However, this is a much more dubious approach to estimating the effects of providing contraception at no cost to the consumer on the rate of unintended pregnancy.
This is because increased contraceptive use does not strictly lead to a lower rate of unintended pregnancy. It is easy to see why. Contraceptive methods just lower the rate of unintended pregnancy; they do not eliminate the chances of pregnancy. There is therefore a race condition when contraceptive use increases.
If there is an increase in sexual intercourse while not desiring pregnancy at the same time that contraceptive use increases, then there can easily be more unintended pregnancies, not less.
This is not just a theoretical concern. As I found in previous analysis, when “the pill” was released in 1960, it backfired spectacularly, leading to an increase in the rate of unintended pregnancy in the 1970s exclusively among contraceptive users. (The rate remained the same among those not using contraception.)
Nonetheless, it is worth exploring this line of thinking.
Starting in 2015, the NSFG started asking women who did not report using a contraceptive method in the current and previous months this question:
If you did not have to worry about cost and could use any type of contraceptive method available, would you want to use a method?
The subsample who were asked this question represented 16,200,000 (±1,300,000) women of reproductive age in the United States not actively using a birth control method.
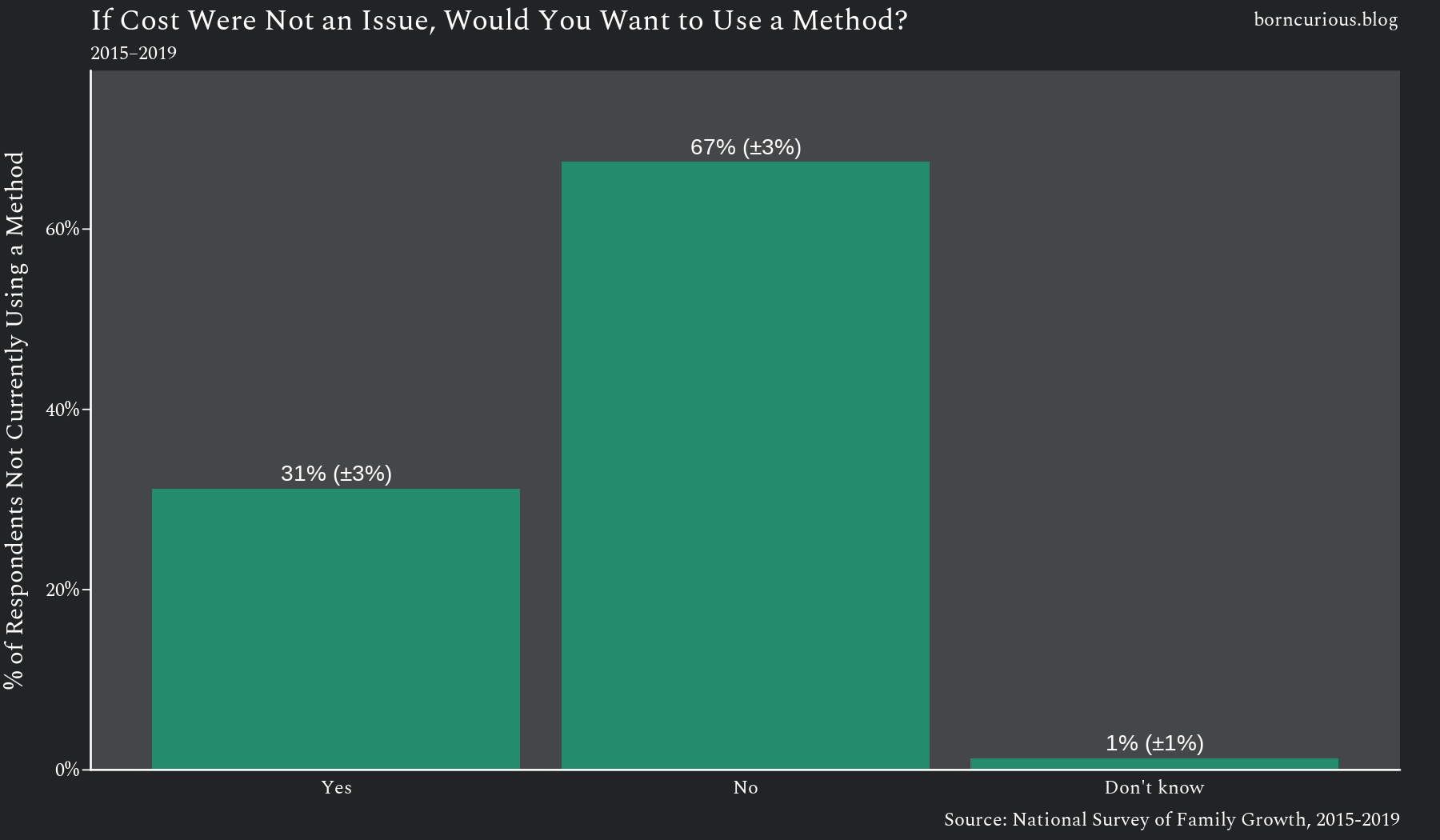
Most answered no.
Still, this question does give proponents of the Lazy Way a little more hope, because the “yes” respondents represent 5,070,000 (±620,000) women. Even if they are a minority of the contraceptive non-users, this is a substantial number of women.
However, this only indicates that there is a (relatively small) demand for free birth control. This should not surprise us. Who does not like getting something for free? This does not necessarily indicate that paying for contraception for these 5 million women would result in fewer unintended pregnancies.
Indeed, given what we learned from women who actually have unintended pregnancies, it is unlikely to have much of any effect.
Does This Hold in 2022–2023?
As I have written previously, the 2022-2023 NSFG data represent a methodological break from previous cycles. Sadly, the data quality appears to be inferior going forward, and results from the pre-2020 cycles and the post-2020 cycles are not directly comparable.
Furthermore, I have not yet calculated weights to adjust for abortion under-reporting for the 2022-2023 data set. I typically make these adjustments to four-year stacked data sets, since two-year data sets have small sample sizes, which can lead to issues with the calculations.
As a check, I ran the estimates from the 2022-2023 data set anyway.
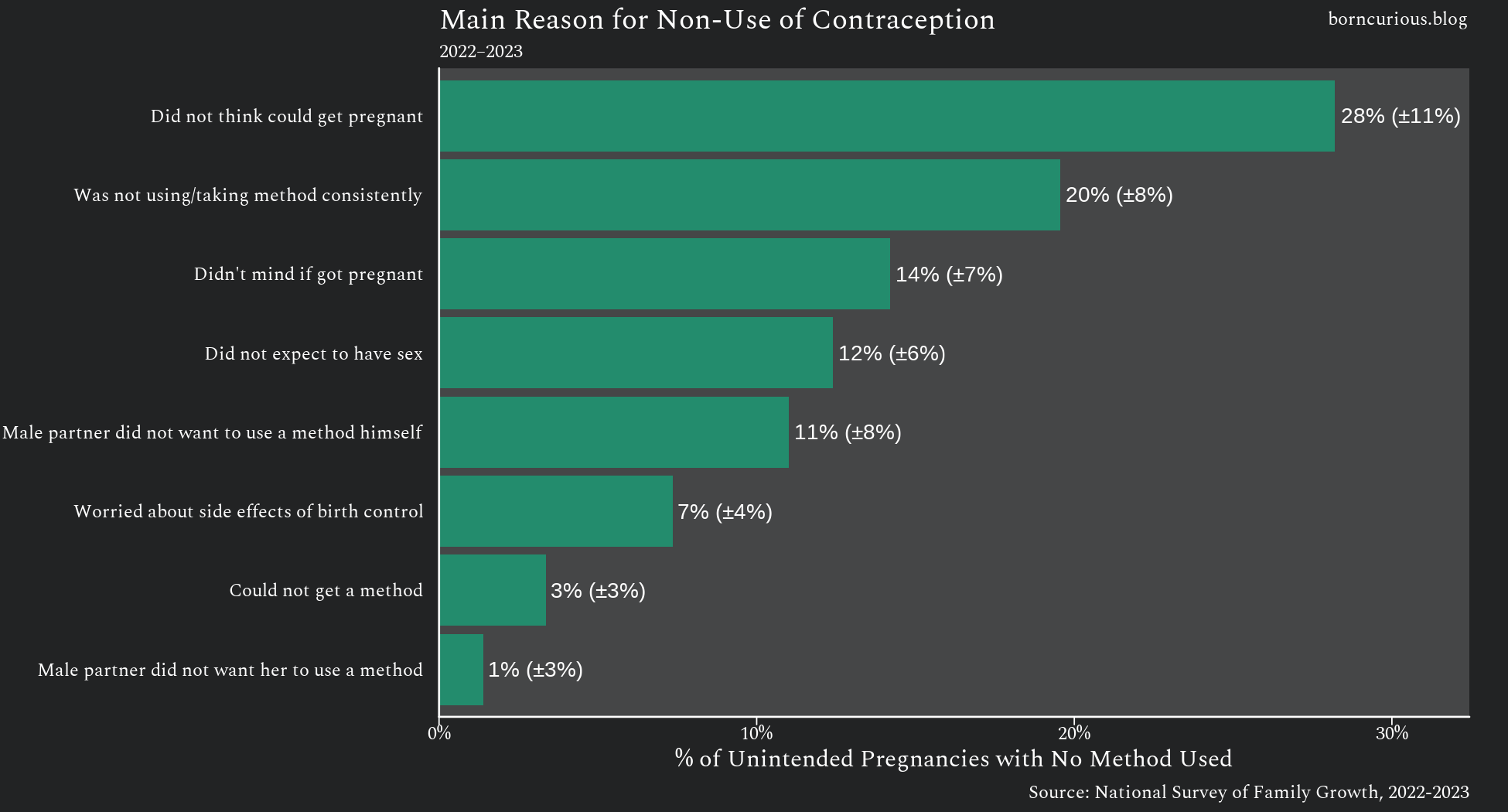
The results are remarkably consistent with previous cycles. Again, “Did not think could get pregnant” was the most common explanation given.
Again, “Could not get a method” was given for a very small fraction of unintended pregnancies, representing 65,800 (±57,800) out of 1,950,000 (±390,000) pregnancies. Indeed, this time its confidence interval barely excluded zero.
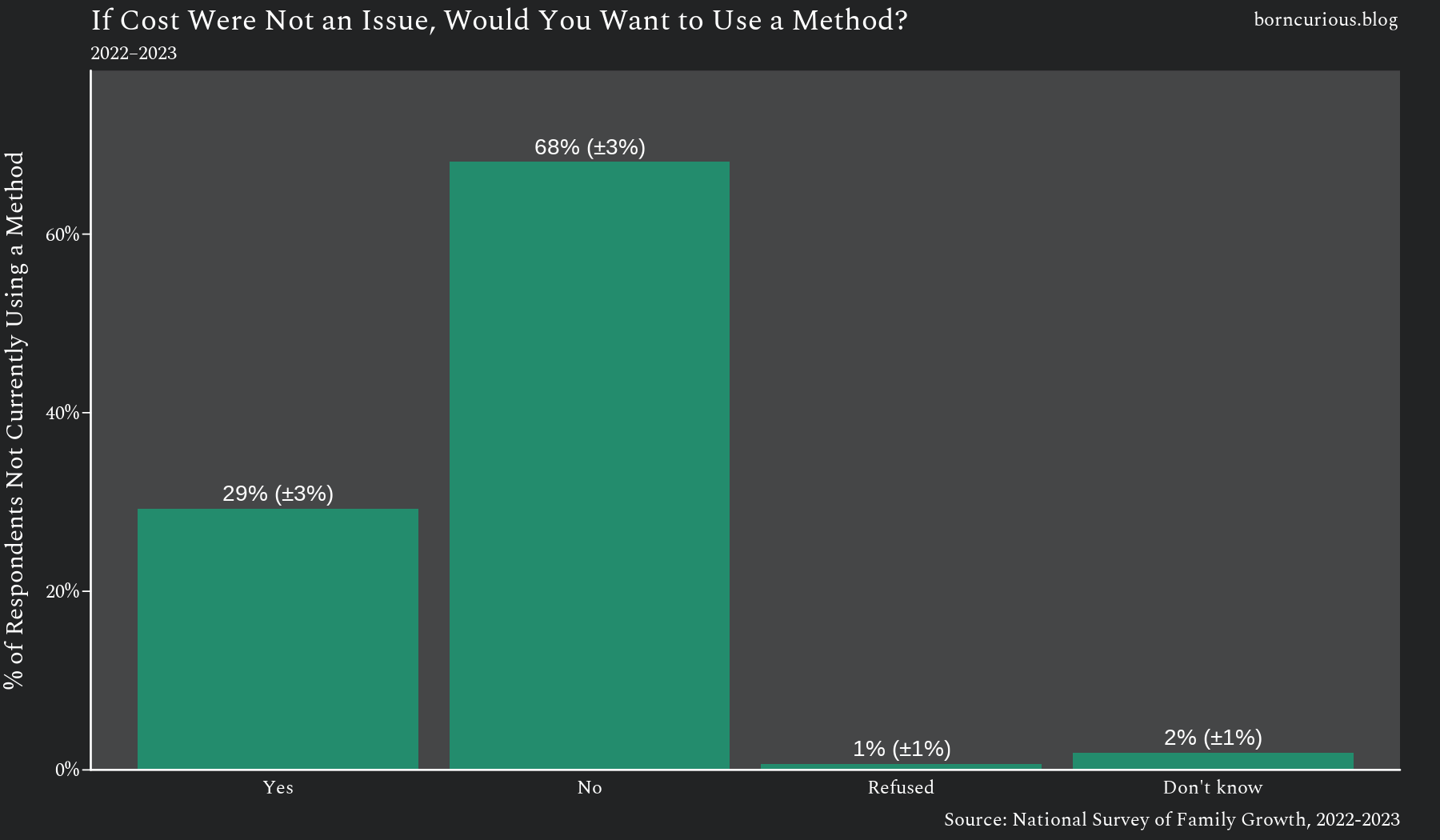
Again, about two-thirds of women not currently using a contraceptive method said they would not even if cost were not an issue.
The fact that these results persist over time and across methodological changes, regardless of whether there is an adjustment for abortion under-reporting, indicates that they are solid.
A Digression on "Couldn't Get Pregnant"
While not the main subject of this analysis, this analysis does raise the question, “Why do about a quarter of women who conceive unintended pregnancies think that they could not have gotten pregnant?”
The NSFG asks a follow-up, free-response question to any woman who gives the “Did not think could get pregnant” response. There is not a dominant answer in these free responses.
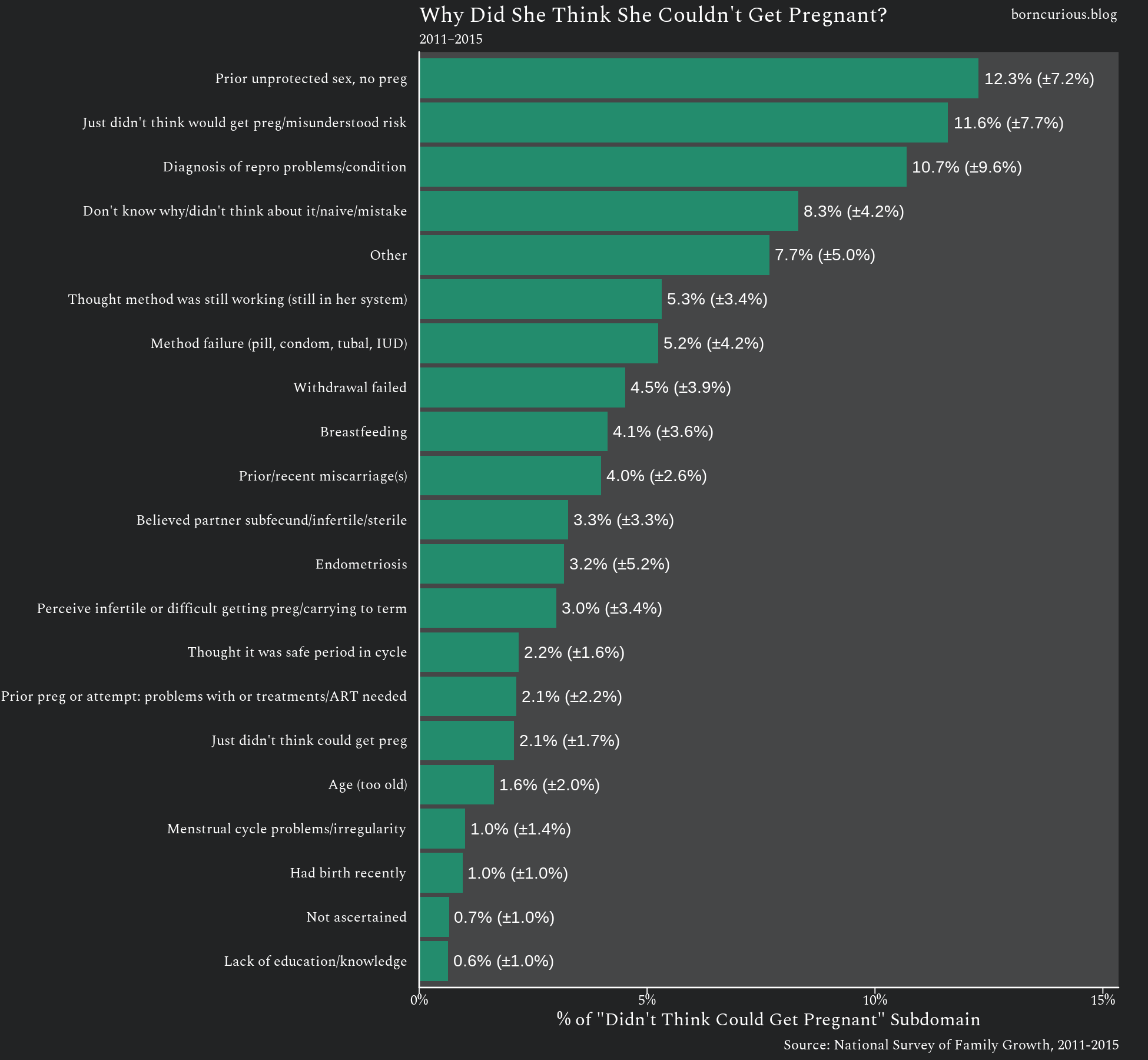
There are many different responses, most with confidence intervals that barely clear zero. None represent a clear plurality. Indeed, some of them like “Just didn’t think would get pregnant” and “Don’t know why” seem to beg the question.
So What About the Hard Way?
If the Lazy Way of passing out contraceptives free of charge is unlikely to have a noticeable effect on the unintended pregnancy rate, then what about the Hard Way?
The contraceptive methods we have today, including the “modern” ones, are prone to failure. The slightly more effective methods often have side effects that deter their use. To top things off, all of these side effects are borne by women. The only reversible methods usable by men are condoms and withdrawal — the same two methods that have been available for centuries.
Therefore, the Hard Way, if it were to produce more effective methods than those currently available, would result in a decline in the unintended pregnancy rate in direct proportion to how much more effective the new methods were and how much of a switch there was from less effective methods to newer ones.5
So, why not the Hard Way?
Grasping at Straws
For one, we do not even know which new methods would work. Basic science research has identified a few potential targets for contraceptive intervention, but none of them are obviously the next big thing.
Indeed, one example of not knowing what new contraceptive method to develop is the 2016 World Health Organization (WHO) trial involving testosterone-based suppression of spermatogenesis, which was canceled due to safety concerns.
Hormonal contraception in women exploits the natural progesterone-induced “off switch” for ovulation that is exercised during menstrual cycling and during pregnancy. Hormonal contraception for women needs only to prevent an ovulation that occurs about once per month by mimicking a hormonal signal that triggers a process that already exists. Even with this low bar, hormonal contraception has a spotty track record for actually working and comes with a whole host of side effects.
There is no such “off switch” for spermatogenesis in men. Indeed, rather than a single ovulation per month, millions of sperm are produced constantly. Each individual sperm takes about two to three months to develop. Hormonal contraception for men, rather than mimicking a pre-existing system, would need to bring this whole spermatogenesis assembly line to a halt for about a quarter of a year to even work.
There was a specious dialogue around these trials regarding double standards for women and men. While there may have been sex-based double standards in other clinical trials, this was not an example of that. Rather, clinical trial standards had become much higher in 2016 than in the 1950s, when many shady practices were used to bring Enovid to market.
Anyone with a basic, textbook knowledge of reproductive physiology could have told you that hormonal suppression of spermatogenesis was a bad idea. The real takeaway from the 2016 WHO trial was, “Wow, they really are grasping at straws, aren’t they?”
A Bad Bet for Pharma
However, there is an even larger issue that makes the Hard Way unlikely. The WHO trial was publicly funded, which helps explain why it happened at all. Bringing a new pharmaceutical to market takes hundreds of millions, if not billions, of dollars. Pharmaceutical companies have been reticent to spend money on research and development of new contraceptives.
Unfortunately, this is understandable in a purely monetary sense. Contraceptives are used predominantly by healthy people, and any pharmaceutical intervention can have side effects. Therefore, with contraceptives, companies expose themselves to the risks of bringing a pharmaceutical to market, without the guarantee of a highly motivated group of consumers that, say, a cancer therapy has.
Therefore, it makes sense for pharmaceutical companies to avoid working on a truly new contraceptive method instead of just repackaging the old ones for the hundredth time. The latter approach has much lower risk and continues to make money.
The "Good Enough" Problem
Anecdotally, if you talk to people in the pharmaceutical industry, you might hear that there is a general sentiment that the existing contraceptives are “good enough.”
This might seem a bizarre sentiment, since we led this article with the observation that there are more than 2 million unintended pregnancies every year in the United States, and many such pregnancies occur among couples using contraception.
This makes more sense when we remember that much of the birth control lobbying and philanthropy shifted from birth control to abortion advocacy in the 1960s and 1970s. The “good enough” attitude might make sense for those who view abortion as the answer to the millions of unintended pregnancies that occur every year.
However, even if this is the conclusion your moral values lead to, it is still a non-sequitur. Slightly less than half of unintended pregnancies end by induced abortion. A simple majority are not. Thus, the “good enough” attitude does not even make sense even if you view abortion as the answer to unintended pregnancy, because it ignores the majority of outcomes for unintended pregnancy.
Conclusion
We identified two ways in which contraception could be an answer to the millions of unintended pregnancies that occur every year. The Lazy Way is to increase access by providing existing birth control methods at little to no cost to the consumer. The Hard Way is to develop new, better methods of contraception.
The Lazy Way has little to no effect. Among women reporting unintended pregnancies who did not use birth control in the month the pregnancy was conceived, a very small proportion (about 5%) report that the main reason they did not use contraception was that they could not get a method. The majority of women who are not currently using a contraceptive method would not start using one if it were provided at no cost.
The Hard Way requires a lot of trial and error, effort, and financial resources — on the order of hundreds of millions to billions of dollars. However, there is insufficient interest to bring this about because pharmaceutical companies see little money to be made against the risk assumed by bringing truly new birth control methods to market and because the values of our philanthropic elite prefer abortion advocacy over costly research and development efforts.
The Lazy Way does not work, and the Hard Way will not happen. Thus, saying contraception will remedy the problem of unintended pregnancy is a dodge, not an answer.
These pregnancies are actually a subset of all the recent, unintended pregnancies in which no birth control method was used. It includes all pregnancies for which no method was used in the entire month in which the pregnancy was conceived. It does not include pregnancies that were conceived without a method, but in a month in which a method was used during other encounters.
In addition to the NSFG instrument’s filtering, I also filtered out those pregnancies for which the respondent volunteered she actually was using a method when the pregnancy was conceived in responses to the WHYNOUSE series.
The difference between the “Worried about side effects of birth control” estimate and the “Could not get a method” estimate is 308,000 (±159,000) pregnancies. The 95% CI excludes zero, so the difference is statistically significant at α = 0.05.
This time, the difference between “Worried about side effects” and “Could not get a method” is not statistically significant. “Worried about side effects of birth control” represents 464,000 (±153,000) pregnancies. The difference between the two is 206,000 (±212,000), and the 95% confidence interval for the difference includes zero.
I do not count the so-called “long-acting reversible contraceptive (LARC)” methods as new methods, as such. They are really new modalities for delivering the old methods. My NSFG-based analysis shows they are of mixed effectiveness, though a few of them do seem more effective than pill modalities. (Research not yet published.)