
Birth Control's Failure
The surge in unintended pregnancies was driven entirely by contraceptive users.
{kind=link}
In previous analyses, I quantified the surge in unintended pregnancies that occurred from 1974 to 1981 in the wake of the so-called “sexual revolution.”
However, that analysis did not resolve the role of birth control in the surge. The question remained, “To what extent does the increase in the unintended pregnancy rate occur among those using contraception versus among those who are not?”
It turns out, all of it.
I did not expect such a clean answer. Most empirical results at the population level are messy and multifactorial.
Contraceptive Users Drove the Entire Surge
The average number of unintended pregnancies per year went from approximately 2.49 million per year to 3.06 million per year, a difference1 of about 566 thousand pregnancies. About 475 thousand of this increase was among contraceptive users, versus about 90 thousand among those not using a birth control method.
However, the 90 thousand increase among non-contraceptive users is within its margin of error of 0, so this supposed difference could be due to sampling variation.
Furthermore, remember that the population was growing during this time frame, as well.
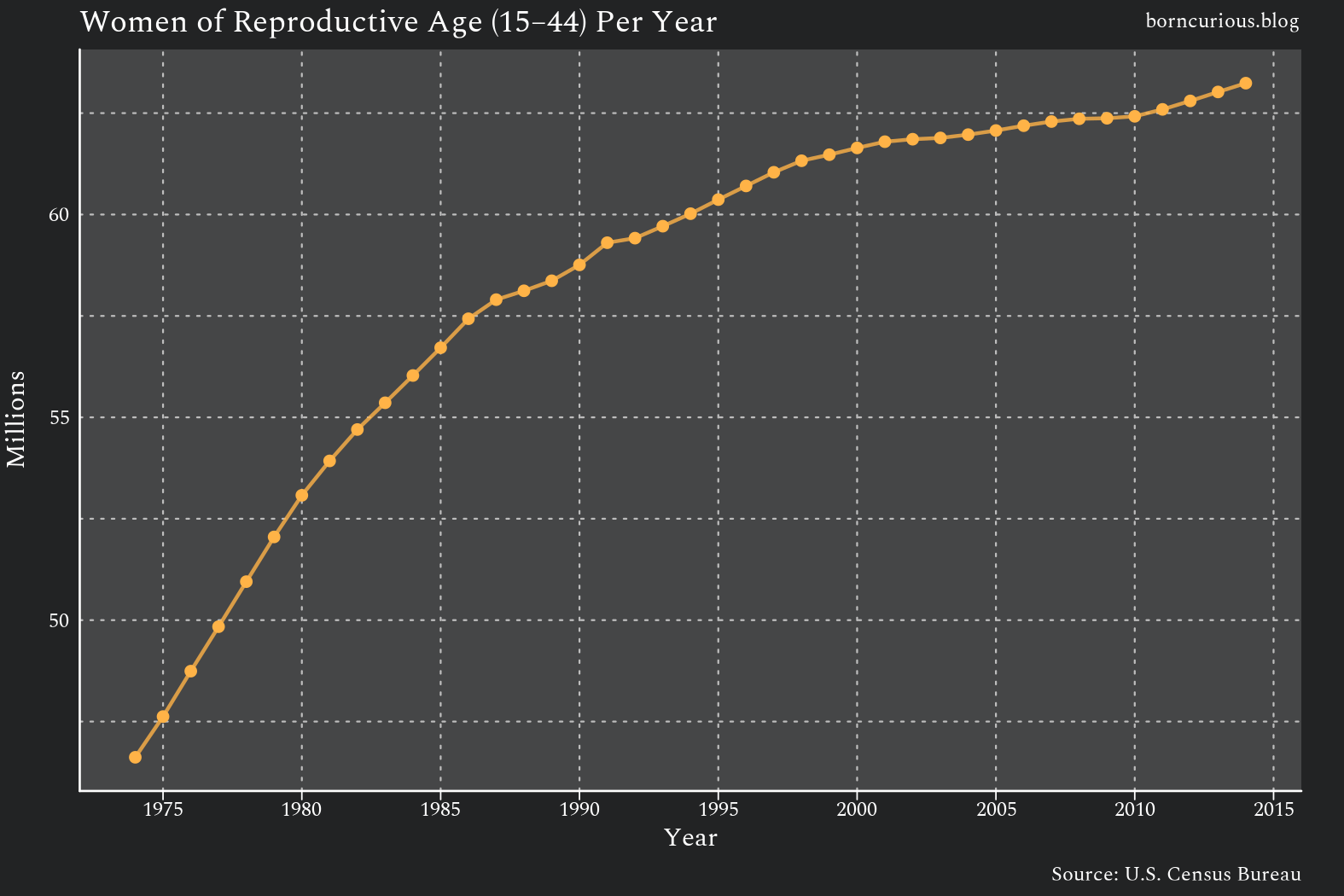
I therefore divided the estimates by the median number of women of reproductive age during each period.
The estimate for the rate of unintended pregnancies among women not using a contraceptive method actually decreased slightly during the surge from 33.1 unintended pregnancies per 1,000 women per year to 32.1, though zero is well within the difference’s margin of error. Thus, we can conclude that the rate of unintended pregnancy among non-users of birth control was basically unchanged.
All of the increase in the unintended pregnancy rate was among contraceptive users, going from 18.6 unintended pregnancies per 1,000 women per year to 26.1.
There were still more unintended pregnancies among non-users than among contraceptive users, but the fact that the surge occurred entirely among users of birth control narrowed this gap quite a bit.
The Pill's Outsize Role
This raises the question, “What methods were being used?”
Cycle 3 of the National Survey of Family Growth (NSFG) asked respondents to report on the contraceptive methods they used in the time interval leading up to the pregnancy.
Respondents could have up to four answers if they changed contraceptive regimes during the period, and each regime could be either a single birth control method or a combination of methods.
I first estimated the percentages of unintended pregnancies for which the various methods were mentioned at least once in the lead-up period, as shown in Table 3.
I found no statistically significant difference in the percentages of pregnancies associated with each method between 1974-1977 and 1978-1981, with only a couple of exceptions,2 so Table 3 includes only the estimates for the whole analysis period.
In the lead-up to unintended pregnancies during contraceptive use, about half of women at least tried the oral contraceptive pill, a greater proportion than any other method.
What about the last method regime mentioned, which is presumably the one used during the conception of the unintended pregnancies?
Looking at Table 4, again, the oral contraceptive pill accounts for the greatest proportion. Indeed, the older methods based on the use of condoms, withdrawal, or calendar timing combined account for fewer unintended pregnancies than the pill.
This is remarkable because hormonal contraceptive pills were the “modern” birth control method in the sexual revolution. Yet the subpopulation experiencing the surge in unintended pregnancies relied on the pill more than any other method.
Discussion
The surge in the rate of unintended pregnancies per woman of reproductive age that occurred in the 1970s occurred entirely among respondents who reported using contraception. Furthermore, the most common method of birth control among those experiencing unintended pregnancies was the oral contraceptive pill.
We, of course, do not know how well respondents were using their birth control methods. Some contraception users could have been using their methods inconsistently. Perhaps some respondents claimed to have been using contraception when they actually were not, due to social desirability bias.
Furthermore, since a much greater proportion of women experiencing unintended pregnancies tried the pill than were using the pill at the time of conception, many women quit the pill, likely due to side effects.
However, as we will see in subsequent analysis, “modern” contraceptive methods are just not as effective as many think, and this gap between expectations and reality likely explains a lot of the surge in unintended pregnancies.
Regardless of the more proximal causes of the contraceptive failures, one striking conclusion emerges from this analysis: the birth control movement was a massive failure.
A Movement That Failed Its Own Goals
The birth control movement promised voluntary motherhood and an end to unintended pregnancies. It also promised — as the modern “family planning” establishment would like you to forget — to put the abortionists out of business. It promised that,
Birth Control will prevent abortion. It will do away with the practice of taking drugs and poisonous nostrums to end undesired pregnancies. It will put an end to the tens of thousands of illegal operations to which women resort in despair. Mothers will not submit to the murder of unborn children when they can control conception. (Sanger 1923)
Those promises did not come to fruition. The oral contraceptive pill — and hormonal birth control more generally — was the last “hurrah” of the birth control movement. The movement's now-maligned founder, Margaret Sanger, even emerged from her retirement to raise funds for the development of the pill. (Eig, 2016)
However, once the pill was actually used by the general population, it led to more unintended pregnancies, not fewer. Rather than bringing induced abortion to an end, it contributed to the surge in the rate of induced abortions in the 1970s, which was driven by the surge in the rate of unintended pregnancies.
Perhaps things could have been different. There were many cultural changes in the 1960s. Perhaps if the pill had been introduced in 1915 instead of 1960, it might have been used more responsibly. This was, at least technically, possible, since a basic understanding of ovulation suppression was already known at the time. (Loeb, 1911)
Alternatively, perhaps the culture has always been such that a technology as flawed as hormonal contraception was going to backfire. These are speculations for which we will never know the truth.
The birth control movement would largely die after the invention of the pill. Alan Guttmacher became president of the Planned Parenthood Federation of America (PPFA) in 1962 and converted the PPFA from a birth control organization to an abortion advocacy organization. Since 1960, no truly new method of birth control has been introduced to the market.3
Sanger witnessed how the birth control movement led by Maria Stritt in Germany in the 1910s went “out of existence” and was replaced by the abortion movement of 1920s Germany. So, too, did the birth control movement in the United States that she founded go out of existence in the 1960s, replaced by the Guttmacher vision of unrestricted abortion. Since then, we have had technological stagnation in contraception.
The birth control movement’s crowning achievement backfired, and the movement failed to achieve its stated goals.
Methodological Issues
Timing of Surge in Unintended Pregnancies
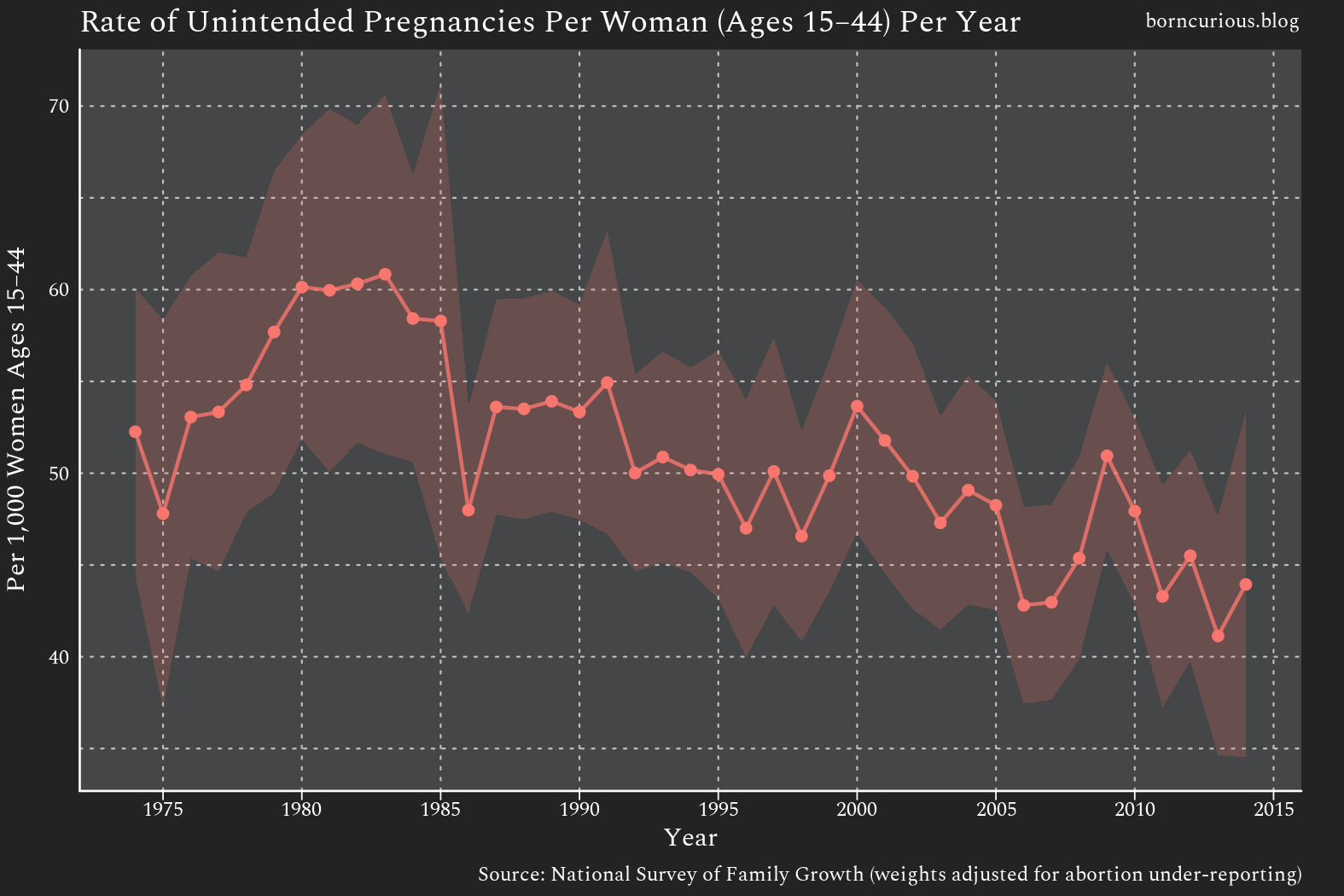
As discussed earlier, my estimates necessarily begin in 1974 due to limitations in data availability. The surge, when adjusted for population growth, plateaus between 1980 and 1981, as seen in Figure 2. I therefore considered the surge period for this analysis to be 1974 to 1981.
Conveniently, this falls entirely within the analysis period for Cycle 3 of the NSFG, so I did not need to harmonize data across surveys.
Contraceptive Use Assessment
To determine whether contraception was used during the time frame in which a pregnancy was conceived, I used the variables C4, C6, C17, and C23 from Cycle 3 of the NSFG.
Both C4 and C17 encode answers to the same question,4
Between (A and B), did you or your partner ever use any method of birth control or family planning for one month or more?
Likewise, C6 and C23 encodes answers to very similar questions,
At the time you became pregnant with (B), had you stopped using all methods of birth control?
and
“Had you stopped using all methods before you became pregnant?
respectively.
I considered a pregnancy to have been conceived during contraception use if the respondent answered “yes” to C4 / C17 and “no” to C6 / C23.
Contraceptive Method Assessment
The NSFG Cycle 3 pregnancy file records the contraceptive methods used during each pre-pregnancy interval through a series of “mention” variables (C5_1M, C5_2M, C5_3M, C5_LM for one interview loop and C18_1M, C18_2M, C18_3M, C18_LM for the other).
These variables encode responses to the question,
Looking at the card and starting with first method you used between (A and B), please tell me the letter for each method used for one month or more in the order you used them.
The variables record methods in chronological order, with C5_1M / C18_1M being the first method used and C5_LM / C18_LM being the last.
Each variable can encode either a single method (codes 1–15, such as pill, condom, or IUD) or a simultaneous pair of methods (codes 16–120, such as “condom + foam”).
Intent Assessment and Pooling for Estimation
A pregnancy was considered unintended exactly as before, and estimates were pooled across four-year intervals due to limitations in sample size. Thus, I compared an average year in 1974-1977 with an average year in 1978-1981.
Citations
Eig, Jonathan. 2016. The Birth of the Pill: How Four Pioneers Reinvented Sex and Launched a Revolution. Pan Macmillan.
Loeb, L. (1911). The Cyclic Changes in the Mammalian Ovary. Proceedings of the American Philosophical Society, 50(199), 228–234.
Sanger, Margaret. 1923. “A Better Race Through Birth Control.” The Thinker, November 1923.
The margin of error (MOE) for the difference appears to be greater than the MOEs for either estimate. That is because the MOE for difference includes a covariance term.
where the covariance is between the sampling errors of the 1974-1977 and 1978-1981 rate estimators. When that covariance is negative (-0.62 correlation here), the - 2*Cov term becomes positive, so you’re adding a third variance component on top of the two individual variances. The difference MOE ends up larger than either individual MOE, because the sampling design makes the two sub-period estimates move in opposite directions: a replicate that pushes one up tends to push the other down, amplifying the swing in their difference.
One of the methods was IUDs, perhaps as a result of the Dalkon Shield scandal going on during this time frame.
There have been new modalities for hormonal contraception, such as injectables and implants, and there have been different chemical analogs of progesterone and estrogens, but these are refinements of the same method.
The only reason there are two variables is that, in the survey instrument, these questions appear in different parts of the script and refer to different pregnancy intervals.